A technique using DNA analysis now enables the identification of more types of bacteria that reside in and on the human body. Interest in the organisms found in the gut, known as the microbiome, has exploded in two directions in recent years. Do they have a part in disease and is there a commercial opportunity? The microbiome appears extensively in research papers and in all types of media and ‘health products’. Suddenly, the microbiome might be responsible for many diseases and needs to be controlled. Why do we have the microbiome, where is it, what is it for and what does it do? Is not easy to find among the barrage of ideas and theories.
The caecum is the first part of the large intestine (colon). Its wall is reinforced by immune tissue from the appendix to along the ascending colon to isolate the microorganisms contained within which are known as the gut microbiome. These organisms are acquired from dietary substances and some will survive in the residues of digestion. This is their only source since birth. The liquid ‘chyme’ from digestion enters the caecum from the small intestine (ileum) via a one-way valve (ileocaecal valve). Any reflux here produces small intestine bacterial overload (SIBO). Symptoms of this are not well defined but pain and bloating and IBS are mentioned.
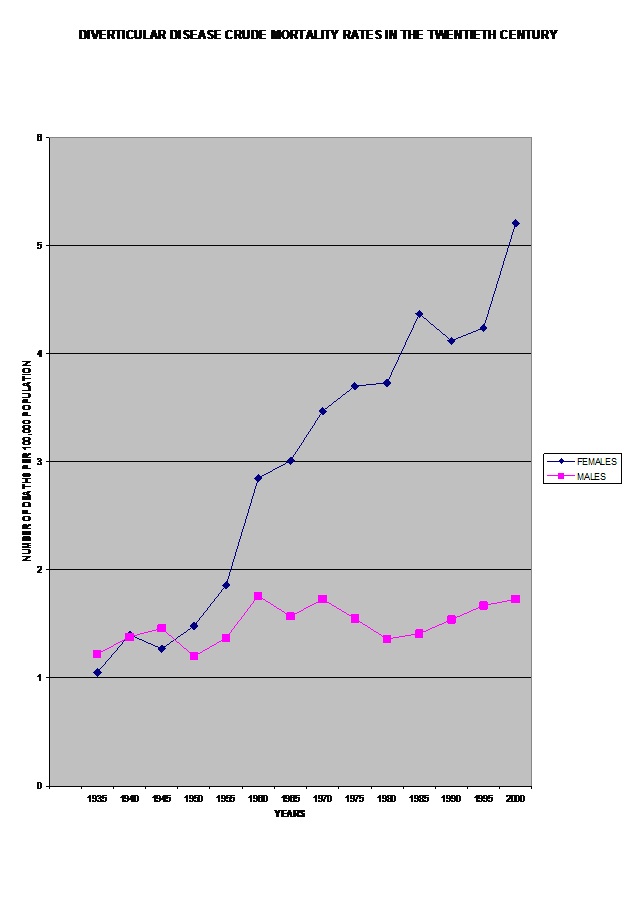
The other import into the caecum microbiome is from the appendix. This is not an evolutionary relic but a safe refuge for the production of live microorganisms to supply and maintain the microbiome if it is depleted. When the output is blocked appendicitis ensues. Being without an appendix appears to increase the risk of infection in diverticular disease.
The liver also uses the food digestion pathway to get rid of detoxification chemicals and those which cannot be passed via the kidneys and urine such as heavy metals and pigments from red blood corpuscles. Bile products from the liver are recycled by the microbiome and returned to the liver for reuse.
When this digestion and body waste enters the caecum it joins the residues of several previous meals and itself will be diluted by several following meals. Colon wall muscles produce mixing movements before slowly advancing the content to the drying phase in the colon and the recycling of water. Because of the slowing of flow in the microbiome, ‘transit time’ from mouth to anus is not related to a complete meal. Similarly, it can take time for the colon to get rid of a toxic organism or irritant.
The array of organisms in the microbiome vary within and between people and are dynamic. They will only be there if they have the right nutrients and conditions to survive. There is an intimate relationship between diet and foodstuffs, and the type of organisms needed to deal with their digestion residues. This system is successful at the extremes of carnivorous or vegetarian diets.
What constitutes an ‘unbalance’ or ‘dysbiosis’ of good and bad bacteria in the microbiome is a human concept, as is the opinion that the microbiome always needs more in number and variety of microorganisms to be effective and healthy. Consider an individual with a restricted diet due to illness found to have a limited range of organisms in their microbiome. This is not dysbiosis but is the microbiome responding to diet. Taking prebiotics, probiotics or fermented food is just changing the diet and too much might not be helpful. Researchers looking for a link between the microbiome and diseases need to consider the effect of the disease on diet. Also, the gut-brain axis is a two-way communication system and neurotransmitter faults in diseases and drugs can also affect colon movement.
There are examples in nature where a lesser species is employed in a symbiotic relationship to solve a problem the host cannot deal with themselves. Powerful enzymes from the pancreas are produced to digest proteins in food but need to be destroyed before they attack the host’s tissues. They cannot be reabsorbed. When a stoma is formed by bringing the end of the small intestine to the outside of the body, the microbiome is not used and the surrounding skin can be attacked by enzymes. A stoma further along the colon, past the microbiome, does not have this problem. Cystic fibrosis patients have to take enzymes to digest their food. Sometimes the microbiome cannot cope with the quantity of enzymes and the ascending colon can be damaged. Only one pancreatic enzyme, elastase, is found in faeces. This is not harmful and is in fact used to show that the pancreas is working.
The microbiome is an integral part of body processes and has self-regulating properties which can be disrupted by pathogenic organisms and antibiotics. The colon itself is controlled by its nerve and blood supply which can change its movements. Not all health problems are caused by the microbiome which is part of an efficient recycling and disposal system which has served mankind for millennia.
© Mary Griffiths 2024
{kind=link}