In the early part of the 20th century constipation was not generally related to any individual illness. The idealised achievement of daily defaecation meant constipation was common particularly in the elderly. Treatment was not free until the NHS came along and natural and herbal laxatives were well used medications. Diverticular disease (DD) became recognised more before WW11. The distinguishing symptoms were pain, fever and diarrhoea. A low residue diet was recommended to reduce diarrhoea and give the bowel rest. Serious pain sometimes resulted in surgery. Infection and inflammation (diverticulitis) were not always present but pieces of food and faeces were trapped in diverticula. Avoidance of coarse fruit and vegetables, seeds and pips was recommended.
Hospital diet sheet for diverticulitis 1961………”forbidden foods – all fried foods, pips and skins of fruits, pastry, suet puddings, coarse stalky vegetables, salads, onions and celery, chunky marmalade, jam with pips or skins, wholemeal or brown bread, coarse biscuits-Ryvita, digestive, Allbran, oatmeal, Weetabix, Shredded Wheat, fruitcake or scones, nuts, dried fruit.”
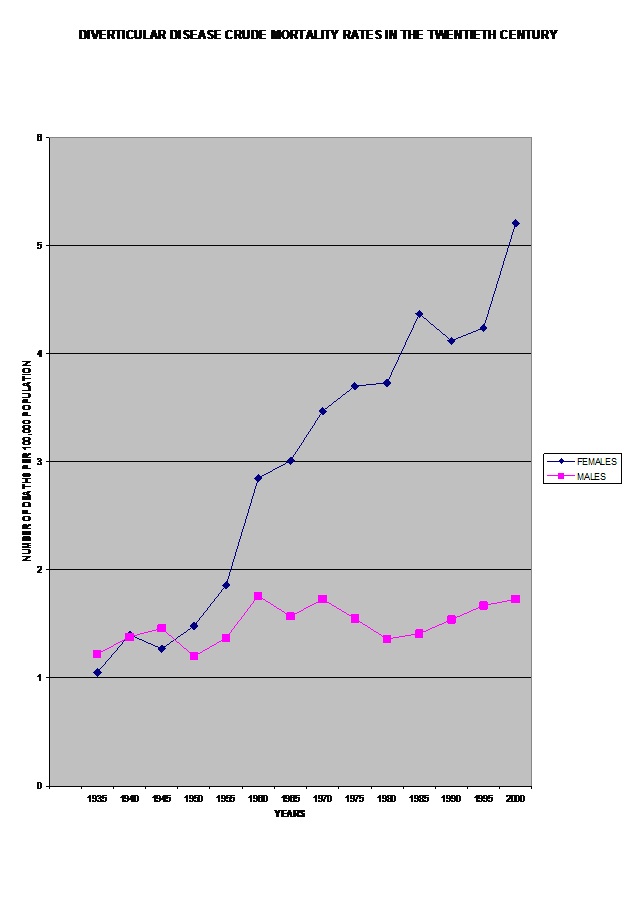
A significant change in diet started about 1970 when treatment for diverticular disease (DD) was suddenly reversed.
Hospital diet sheet for diverticulis 1982………..”you can eat a normal varied diet but include…… (all of the forbidden foods from 1961 except fried food)….SUPPLEMENT meals with 2 teaspoonfuls of unprocessed bran twice daily. EAT LESS white flour in any form and white and other sugars. DIETARY FIBRE ….by helping to restore normal function of the digestive tract, fibre can be useful in the treatment of constipation and diarrhoea”
- Who persuaded health professionals that wheat bran was good for diarrhoea?
- What was the evidence for this complete reversal of treatment?
- Did anyone ask patients if this helped them?
- Who was behind this change?
{kind=link}